When you buy through our links, we may earn a commission. Products or services may be offered by an affiliated entity. Learn more.

Parasomnias


- Parasomnias are a group of sleep disorders that involve unusual behaviors, movements, emotions, or experiences that occur while falling asleep, during sleep, or when waking up.
- Common parasomnias include sleepwalking, sleep talking, night terrors, nightmares, REM sleep behavior disorder, and confusional arousals.
- Parasomnias can affect both children and adults and may be triggered by factors such as sleep deprivation, stress, medications, certain medical conditions, or other sleep disorders.
- While many parasomnias are harmless, frequent episodes, injuries, or potentially dangerous behaviors should be evaluated by a healthcare provider or sleep specialist.
Unusual behaviors during sleep — sleepwalking, sleep talking, or acting out dreams — can be unsettling, but they’re more common than many people realize. These experiences are known as parasomnias. Some parasomnias are harmless and tend to resolve on their own, particularly in children, while others may increase the risk of injury or signal an underlying sleep or medical condition.
Below, we’ll explain the different types of parasomnias, their symptoms and causes, and when treatment or a medical evaluation may be needed.
Looking to improve your sleep? Try upgrading your mattress.

What Is a Parasomnia?
Parasomnias are a group of sleep disorders that involve unusual movements, behaviors, emotions, or perceptions while falling asleep, during sleep, or as you wake up . Most people experience parasomnias at some point in life.
If you’ve ever talked in your sleep, sleepwalked, or woken up with your heart racing after a frightening dream, you’ve experienced a parasomnia. In most cases, parasomnias are not harmful. But, they may be disturbing or frustrating. In some cases, parasomnia activity can be dangerous to sleepers or their bed partners, or a symptom of an underlying medical condition.
Causes of Parasomnias
Not all parasomnias have a clear cause, but researchers have identified several potential causes and triggers for parasomnias.
- Sleep deprivation: If you don’t get enough sleep, you’re more likely to experience parasomnias . This may be because sleep deprivation can alter the stages of sleep .
- Disturbed sleep: Frequent nighttime sleep disruptions can provoke parasomnias. If you have a condition that disturbs sleep, such as sleep apnea, restless legs syndrome, or chronic pain, you may be more vulnerable to parasomnias.
- Stress: If you are feeling stress or anxiety, or if a negative life event has recently affected you, you may experience parasomnias .
- Psychological disorders: Research has linked depression, post-traumatic stress disorder (PTSD), and other mental health conditions to parasomnias.
- Neurological disorders and diseases: Conditions that affect the nervous system can cause parasomnias. These include narcolepsy, multiple sclerosis, Parkinson’s disease, dementia, brain tumors, and more.
- Medications: Some medications may make parasomnias more likely, including certain antidepressants.
- Inherited traits: Genes play a role in some parasomnias, so if you have a family history of a certain parasomnia, you may be more likely to experience them.
Types of Parasomnias
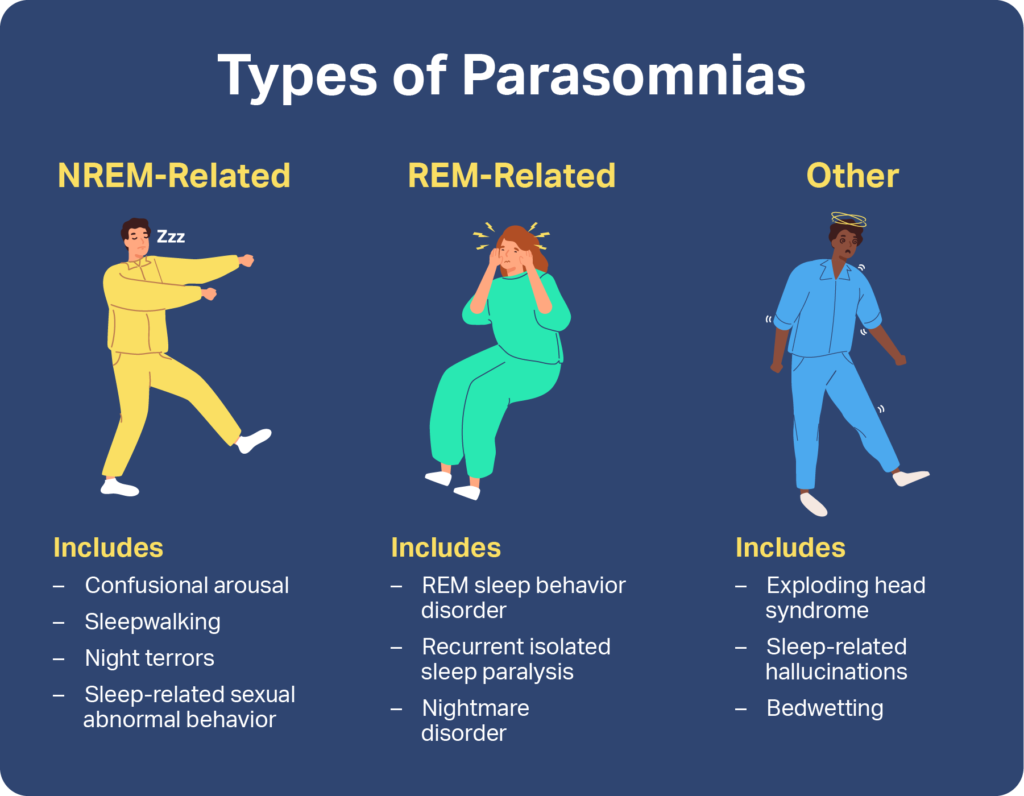
Sleep experts classify parasomnias by the stages of sleep they occur during. Some are associated with non-rapid eye movement (NREM) sleep, which encompasses the first three stages of sleep, while others happen during rapid eye movement (REM) sleep. Other parasomnias may occur during any sleep stage or during the transition into or out of wakefulness.
NREM Parasomnias
The parasomnias that happen during NREM sleep are often described as “disorders of arousal.” People who experience them partially wake up. Their eyes may be open, and they may appear to act with intention. However, they may not respond when spoken to, and they may have no memory of what happened afterward . NREM-related parasomnias tend to be more common in children .
")



REM Parasomnias
REM-related parasomnias occur during rapid eye movement (REM) sleep or in the transition out of it. These parasomnias tend to occur in the final hours of a night’s sleep, often very early in the morning. Unlike non-REM parasomnias, individuals can usually remember these episodes.





Other Parasomnias
Some parasomnias are not associated with NREM or REM sleep, because they can happen at any time during sleep or they happen when a person is falling asleep or waking up. Sleep experts classify these behaviors and events as “other parasomnias.”



Treatment for Parasomnias
Treatment for parasomnias can vary depending on the type of parasomnia and its cause. Some parasomnias require no treatment, while doctors may recommend managing others with:
- Healthy sleep habits
- Stopping or stopping certain medications
- Therapy
- Relaxation techniques
If you or someone in your care is experiencing parasomnias, talk to a doctor. A medical professional can help you manage symptoms, improve sleep, and stay safe throughout the night.

Still have questions? Ask our community!
Join our Sleep Care Community — a trusted hub of sleep health professionals, product specialists, and people just like you. Whether you need expert sleep advice for your insomnia or you’re searching for the perfect mattress, we’ve got you covered. Get personalized guidance from the experts who know sleep best.
Lucy Bryan is a writer and editor with more than a decade of experience in higher education. She holds a B. A. in journalism from the University of North Carolina at Chapel Hill and an M.F.A. in creative writing from Penn State University.
Dustin Cotliar, MD, holds a medical degree from the State University of NY (SUNY) Downstate College of Medicine, and a master’s in public health from Columbia University, where he focused on healthcare policy and management. He is board-certified in Emergency Medicine, with over eight years of practice that includes emergency medicine, urgent care, and telemedicine.
Learn more about our medical advisory boardReferences7 Sources
Alshahrani, S. M., Albrahim, R. A., Abukhlaled, J. K., Aloufi, L. H., & Aldharman, S. S. (2023). Parasomnias and associated factors among university students: A cross-sectional study in Saudi Arabia. Cureus, 15(11), e48722.
https://pubmed.ncbi.nlm.nih.gov/38094542Singh, S., Kaur, H., Singh, S., & Khawaja, I. (2018). Parasomnias: A comprehensive review. Cureus, 10(12), e3807.
https://pubmed.ncbi.nlm.nih.gov/30868021/Kirsch, D. (2023, July 25). Stages and architecture of normal sleep. UpToDate.
https://www.uptodate.com/contents/stages-and-architecture-of-normal-sleepVaughn, B. V. (2024, June 11). Approach to abnormal movements and behaviors during sleep. UpToDate.
https://www.uptodate.com/contents/approach-to-abnormal-movements-and-behaviors-during-sleepZak, R., & Karippot, A. (2023, October 18). Nightmares and nightmare disorder in adults. UpToDate.
https://www.uptodate.com/contents/nightmares-and-nightmare-disorder-in-adultsA.D.A.M. Medical Encyclopedia [Internet]. (2023, April 28). Night terrors in children. MedlinePlus.
https://medlineplus.gov/ency/article/000809.htmMainieri, G., Loddo, G., & Provini, F. (2021). Disorders of arousal: A chronobiological perspective. Clocks & Sleep, 3(1), 53–65.
https://pubmed.ncbi.nlm.nih.gov/33494408/