When you buy through our links, we may earn a commission. Products or services may be offered by an affiliated entity. Learn more.

Mental Health and Sleep


- Mental health impacts thoughts, feelings, and actions and influences our ability to handle stress, relate to others, and make choices.
- Quality sleep is crucial for good mental health, but sleep issues can worsen mental health conditions, and mental health problems can lead to poor sleep.
- Adhering to sleep hygiene practices can improve sleep quality and mental well-being.
Most people know firsthand that sleep affects their mental state. After all, there’s a reason it’s said that someone in a bad mood “woke up on the wrong side of the bed.”
As it turns out, there’s quite a bit of truth behind this colloquial saying. Sleep is closely connected to mental and emotional health and has demonstrated links to depression, anxiety, bipolar disorder, and other conditions.
Research is ongoing to better understand the bidirectional relationship between mental health and sleep. Both are complex issues affected by a multitude of factors, but, given their close association, there is strong reason to believe that improving sleep can have a beneficial impact on mental health and can be a component of treating many psychiatric disorders.
How Is Mental Health Related to Sleep?
Brain activity fluctuates during sleep, increasing and decreasing during different sleep stages that make up the sleep cycle. Each stage plays a role in brain health, allowing activity in different parts of the brain to ramp up or down and enabling better thinking, learning, and memory. Research has also uncovered that brain activity during sleep has profound effects on emotional and mental health.
Sufficient sleep, especially rapid eye movement (REM) sleep, facilitates the brain’s processing of emotional information. During sleep, the brain works to evaluate and remember thoughts and memories, and it appears that a lack of sleep is especially harmful to the consolidation of positive emotional content. This can influence mood and emotional reactivity and is tied to mental health disorders and their severity, including the risk of suicidal ideas or behaviors.
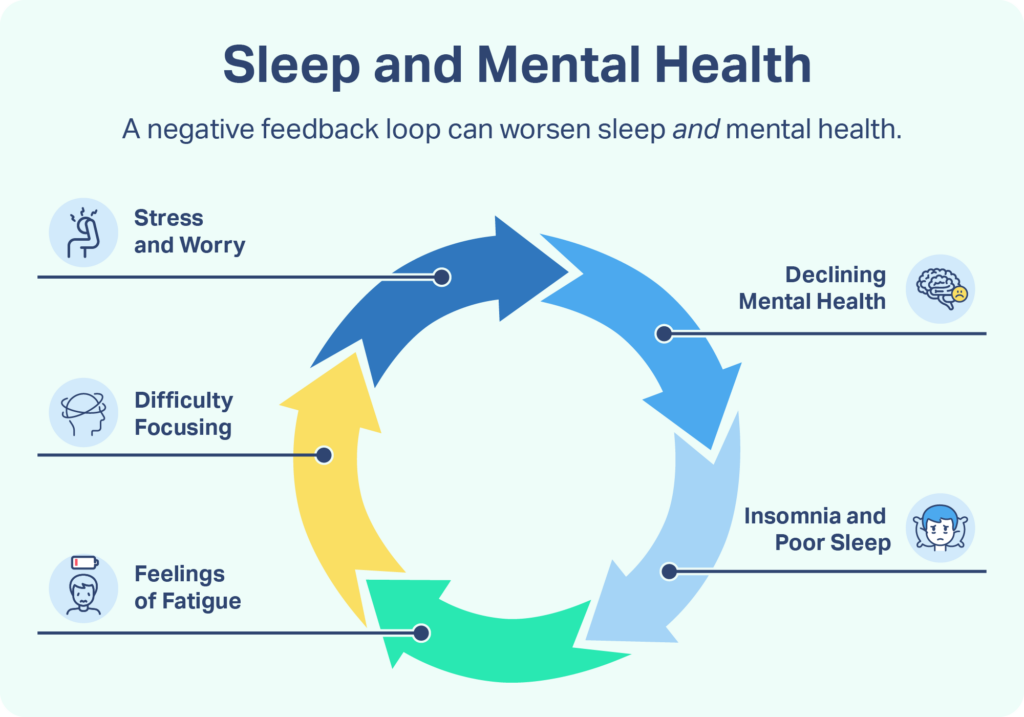
As a result, the traditional view, which held that sleep problems were a symptom of mental health disorders, is increasingly being called into question. Instead, it is becoming clear that there is a bidirectional relationship between sleep and mental health in which sleeping problems may be both a cause and consequence of mental health problems. Further research is needed to identify the diverse connections between sleep and mental health as well as how their multifaceted relationship can be influenced by numerous factors in any specific person’s case.
Obstructive sleep apnea (OSA) is another aspect of sleep that has been linked to mental health. OSA is a disorder that involves pauses in breathing during sleep and a reduction in the body’s oxygen levels, creating fragmented and disturbed sleep. OSA occurs more frequently in people with psychiatric conditions and may detract from their physical health and heighten their risk of serious mental distress.


")

Sleep and Specific Mental Health Problems
The way that sleep and mental health are intertwined becomes even more apparent by reviewing what is known about how sleep is tied to a number of specific mental health conditions and neurodevelopmental disorders.








Ways To Improve Both Sleep and Mental Health
This multifaceted relationship between sleep and mental health makes for complex connections between sleep and psychiatric disorders, but it also means that treatment for both issues can go hand-in-hand. Steps to improve sleep may even form part of a preventive mental health strategy.
Every individual’s situation is different, so the optimal treatment for mental health and sleep problems depends on the person. Because these conditions can have a major impact on quality of life, it’s important to receive proper care, which entails working with a trained health professional.
A medical doctor or psychiatrist can review the potential benefits and risks of different types of treatments and provide tailored care – even in situations with multiple co-occurring physical or mental health issues.
Cognitive Behavioral Therapy
Cognitive behavioral therapy (CBT) describes a type of counseling known as talk therapy. It works by examining patterns of thinking and working to reformulate negative thoughts in new ways. For many patients, help from a trained counselor to reframe their thinking can meaningfully improve both their sleep and mental state.
Different types of CBT have been developed for specific problems such as depression, anxiety, and bipolar disorder. In addition, CBT for insomnia (CBT-I) has a proven track record in reducing sleeping problems. A large clinical trial also showed that CBT-I could reduce symptoms of many mental health conditions, improving emotional well-being and decreasing psychotic episodes.
")
Improve Sleep Habits
A common cause of sleeping problems is poor sleep hygiene. Stepping up sleep hygiene by cultivating habits and a bedroom setting that are conducive to sleep can go a long way in reducing sleep disruptions.
Examples of steps towards healthier sleep habits include:
- Having a set bedtime and maintaining a steady sleep schedule
- Finding ways to wind-down, such as with relaxation techniques, as part of a standard routine before bedtime
- Avoiding alcohol, tobacco, and caffeine in the evening
- Dimming lights and putting away electronic devices for an hour or more before bed
- Getting regular exercise and natural light exposure during the daytime
- Maximizing comfort and support from your mattress, pillows, and bedding
- Blocking out excess light and sound that could disrupt sleep
Finding the best routines and bedroom arrangement may take some trial and error to determine what’s best for you, but that process can pay dividends in helping you fall asleep quickly and stay asleep through the night.

Still have questions? Ask our community!
Join our Sleep Care Community — a trusted hub of sleep health professionals, product specialists, and people just like you. Whether you need expert sleep advice for your insomnia or you’re searching for the perfect mattress, we’ve got you covered. Get personalized guidance from the experts who know sleep best.
Eric Suni has over a decade of experience as a science writer and was previously an information specialist for the National Cancer Institute.
Dr. Alex Dimitriu is the founder of Menlo Park Psychiatry and Sleep Medicine. He is board-certified in psychiatry as well as sleep medicine.
Learn more about our medical advisory boardReferences3 Sources
Bernert, R. A., Kim, J. S., Iwata, N. G., & Perlis, M. L. (2015). Sleep disturbances as an evidence-based suicide risk factor. Current psychiatry reports, 17(3), 554.
https://pubmed.ncbi.nlm.nih.gov/25698339/Knechtle, B., Economou, N. T., Nikolaidis, P. T., Velentza, L., Kallianos, A., Steiropoulos, P., Koutsompolis, D., Rosemann, T., & Trakada, G. (2019). Clinical Characteristics of Obstructive Sleep Apnea in Psychiatric Disease. Journal of clinical medicine, 8(4), 534.
https://pubmed.ncbi.nlm.nih.gov/31003451/Freeman, D., Sheaves, B., Goodwin, G. M., Yu, L. M., Nickless, A., Harrison, P. J., Emsley, R., Luik, A. I., Foster, R. G., Wadekar, V., Hinds, C., Gumley, A., Jones, R., Lightman, S., Jones, S., Bentall, R., Kinderman, P., Rowse, G., Brugha, T., Blagrove, M., … Espie, C. A. (2017). The effects of improving sleep on mental health (OASIS): a randomised controlled trial with mediation analysis. The lancet. Psychiatry, 4(10), 749–758.
https://pubmed.ncbi.nlm.nih.gov/28888927/